You are here : Home / Infertility Investigations for Male and Female before Undertaking Fertility Treatments
Text :
Infertility Investigations for Male and Female before Undertaking Fertility Treatments
Introduction
The basic infertility investigation is done when you begin your treatment and is usually arranged right after your initial consultation. A basic infertility investigation involves testing of three things: the 'woman's hormone status (day 3 blood work), a test of the Fallopian tubes, and a sperm count. The whole basic infertility investigation is completed in one cycle.
USG
A vaginal ultrasound is very useful in infertility because it allows a detailed examination of the uterus and ovaries. A vaginal ultrasound involves the use of a vaginal probe and is best done with an empty bladder. In ultrasound several things will be evaluated. Uterine size and shape can be assessed, as can the presence of fibroids, polyps and adenomyosis. The ovaries can be extremely well seen with vaginal ultrasound. The size of the ovaries is very important in infertility evaluation. The larger volume & increased stromal thickness is often due to multiple small cysts or follicles and this is what gives polycystic ovaries their name. Smaller ovarian volumes are often associated with a decreased ovarian reserve or fewer eggs. This assessment is very important in older women. The number of small follicles (antral follicles) present helps us to predict how far along this "road" your ovaries are. The antral follicle count (AFC) is thought to be as predictive for the number of eggs left as the day three FSH level. Ovarian cyst can usually be seen easily with ultrasound. As you cycle each month, an egg or eggs are matured in a follicle. A follicle is an ovarian cyst. It can look like any other ovarian cyst except in changes quickly during your cycle and is usually present for only one cycle. Sometimes the only indication of endometriosis is an ovarian cyst called an endometrioma which is first seen on this vaginal ultrasound. Sometimes, begin (not cancers) ovarian umors can also be detected. Of course, the first signs of full vary in cancer can also be seen on this ultrasound but this finding would be exceedingly rare. If the cyst is found on ultrasound, at a few months of observation to see if it goes away may be suggested or a laparoscopy may be suggested to establish the diagnosis.
Hysterosonograms
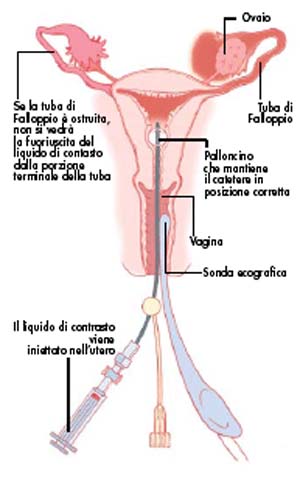
Saline infusion hysterosonograms is the test of choice to confirm pathology within the endometrial cavity. Sonohysterosonograms can also be done with contrast material (contrast hysyerosonogram) to deternine if the fallopian tubes are open. Hysterosalingogram still remain the standard of care as far as demonstrationg the tubes to be open but this test may replace it in the future. The advantage of this test is that it avoids any x-ray exposure.
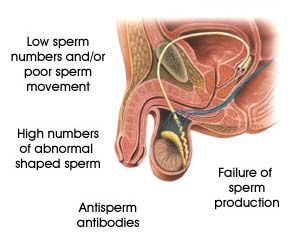
Seminal Assay
Semen analysis is an integral part of the workup of couples consulting for infertility. The availability of semen renders possible direct examination of male germ cells. Semen analysis includes the examination of:
Spermatozoa
Other cells present in semen
Seminal fluid
Altogether these data give indications on the testicular function and of the integrity of the male genital tract. Definitions of terminology used when describing semen sample
Normozoospermia
When all the spermatozoal parameters are normal together with normal seminal plasma, WBC’s and there is no agglutination.
Oligozoospermia
When sperm concentration is < 20 million/ml.
Asthenozoospermia
Fewer than 50% speromatozoa with forward progression (categories (a) and (b) or fewer than 25% spermatozoa with category (a) movement.
Teratozoospermia
Fewer than 50% spermatozoa with normal morphology.
Oligoasthenoteratozoos permia
Signifies disturbance of all the three variables (combination of only two prefixes may also be used).
Azoospermia
No spermatozoa in the ejaculate.
Aspermia
No ejaculate.
It should be emphasized that semen is an exception amongst biological fluids since its parameters display very wide intra and inter-individual variations. Therefore semen analysis should be repeated to take intra-individual variations over time into account and confirm abnormal parameters.
Normal values of semen variables (WHO Guidelines)
Standard tests
Normal values
Volume
2.0 ml or more
pH
7.2-7.8
Sperm concentration
20x106 spermatozoa/ml or more
Total sperm count
40x106 spermatozoa or more
Motility
50% or more with forward progression or 2.5% or more with rapid progression within 60 min after collection
Morphology
30% or more with normal morphologyb
Vitality
75% or more live
White blood cells
Fewer than 1x106/ml
Immunological tests
Immunobead test
Fewer than 20% spermatozoa with adherent particles
Basic Information
Person coming for seminal assay should have abstained from sexual activity from 3-5 days.
Sample should be given at the hospital premises ; special cubicles are available for this purpose.
Outstation patients traveling from long distances should rest for 2 hrs before producing a sample, or if possible, to come over to Bangalore the day before giving the sample. This is to avoid stress and strain as it could lead to improper collection and subsequent wrong report.
Anyone who wants assistance from wife may take up a room for a short while.
Both partners are tested for HbsA g & HIV I & HIV II.
Time of collection : 11 am to 1 pm as otherwise the procedure will not be complete before lab closes.
Hysterosalpingogram
A normal hysterosalpingogram. Note the catheter entering at the bottom of the screen, and the contrast medium filling the uterine cavity (small triangle in the center).
Definition : Hysterosalpigography is a procedure where x rays are taken of a woman's reproductive tract after a dye is injected. Hystero means uterus and salpingo means tubes, so hysterosalpigography literally means to take pictures of the uterus and fallopian tubes. This procedure may also be called hysterography ( or HSG).
Hormonal assays
Hormonal
assay examination
Target organ and hormone
Procedure
Rationale
Pituitary
gonadotropins
FSH and LH levels.
Blood serum measurement.
Taken days 2-6 of menstrual cycle.
May help to rule out ovarian
failure.
Abnormal levels of FSH and LH may indicate infertility due to
hyperprolactinaemia LH-FSH ratio may be useful in PCOS diagnosing
and selecting proper therapy.
Prolactin
Prolactin levels.
Blood serum measurement
taken.
Usually taken days 2-6 of menstrual cycle.
High levels of prolactin
(hyperprolactinaemia) can indicate the presence of pituitary tumour
and can cause /menstrual ovulation disorder.
Hyperprolactinaemia blocks the action of LH and FSH.
Ovary
Oestradiol (E2) levels.
Blood serum measurement
taken.
Usually taken days 2-6 of menstrual cycle.
Used to assess ovarian
function.
Oestradiol levels can be used to monitor follicular
development.
Ovary
Testosterone (T) levels.
Blood serum measurement.
Provides evidence of the
occurrence of ovulation.
Ovary
Progesterone (P) levels.
Blood serum measurement, taken at
day 21 of the menstrual cycle (7 days post ovulation).
Usually taken days 2-6 of cycle. Dexamethasone suppression.
Used as an assessment of androgen
production.
Abnormally elevated androgen levels may be a factor for
infertility in females.
Abnormally deficient testosterone levels may lead to infertility
in males.
Can determine the site of excess androgen production.
Thyroid
Thyroid function tests (TSH, T3, T4).
Blood tests to determine total
serum thyroxine (T4), TSH and TRH.
To detect hypothyroidism (a
deficiency of thyroid activity) that may lead to infrequent
ovulation.
As can be seen from this table, it is very
important to conduct certain tests within the infertility
evaluation at a particular time during the woman's menstrual cycle
for the results to be valid.
Day 3 - FSH
The level of FSH is controlled by a complex interactionof several hormones. High levels of FSH on day 3 of the menstrual cycle may indicate the onset of menopause. The injectable FSH medications given to stimulate ovulation mimic the bodies natural FSH. Artificilly raising FSH levels with medication (ovulation induction) during the first part of the ovulatory cycle causes the development of multiple eggs, which are needed for assisted reproductive procedure, such as IVF.
FSH should be measured in all women to exlude premenopause. Depending on the laboratory, an FSH level greater than 10 mIU/ml may be of concern. FSH is tested to see if 1. Patient will respond to the normal line of treatment, 2. Is a good indicator of functional ovarian reserve, 3. will detect menopausal levels.
Purpose
Hysterosalpingography is used to determine if the fallopian tubes are open, or if there are any apparent abnormalities or defects in the uterus. It can be used to detect tumors, scar tissue, or tears in the lining of the uterus. This procedure is often used to help diagnose infertility in women. The fallopian tubes are the location where an egg from the ovary joins with sperm to produce a fertilized ovum. If the fallopian tubes are blocked or deformed, the egg may not be able to descend or the sperm may be blocked from moving up to meet the egg. Up to 30% of all cases of infertility are due to damaged or blocked fallopian tubes.
Preparation
This procedure is generally done in the x-ray department of a hospital or large clinic. General anesthesia is not needed. A pain reliever may be taken prior to the procedure to lessen the severity of cramping.
Description
As with other types of pelvic examinations, the woman will lie on her back on an examination table with her legs sometimes raised in stirrups. The x-ray equipment is placed above the abdomen.
A speculum is inserted into the vagina and a catheter (a thin tube) is inserted into the uterus through the cervix (the opening to the uterus). A small balloon in the catheter is inflated to hold it in place. A liquid water-based or oil-based dye is then injected through the catheter into the uterus. This process can cause cramping, pain, and uterine spasms.
As the dye spreads through the reproductive tract, the doctor may watch for blockages or abnormalities on an x-ray monitor. Several x rays will also be taken. The procedure takes approximately 15-30 minutes. The x rays will be developed while the patient waits, but the final reading and interpretation of the x rays by a radiologist (a doctor who specializes in x rays) may not be available for a few days.
Interestingly, sometimes the hysterosalpingography procedure itself can be considered a treatment. The dye used can sometimes open up small blockages in the fallopian tubes.
Aftercare
The woman is observed for some period after the procedure to ensure that she does not have any allergic reactions to the dye. A sanitary napkin may be worn after the procedure to absorb dye that will flow out through the vaginal opening. If a blockage is seen in a tube, the patient may be given an antibiotic. A woman should notify her doctor if she experiences excessive bleeding, extensive pelvic pain, fever, or an unpleasant vaginal odor after the procedure. These symptoms may indicate a pelvic infection. Counseling may be necessary to interpret the results of the x rays, and to discuss any additional procedures to treat tubal blockages or uterine abnormalities found.
Risks
Cramps during the procedure are common. Complications associated with hysterosalpingography include abdominal pain, pelvic infection, and allergic reactions. It is also possible that abnormalities of the fallopian tubes and uterus will not be detected by this procedure.
Normal results
A normal hysterosalpingography will show a healthy, normally shaped uterus and unblocked fallopian tubes.
Abnormal results
Blockage of one or both of the fallopian tubes or abnormalities of the uterus may be detected.
For more information, medical assessment and medical quote
send your detailed medical history and medical reports
as email attachment to
Em@il : - info@wecareindia.com
Call: +91 9029304141 (10 am. To 8 pm. IST)
(Only for international patients seeking treatment in India)
You are here : Home / Infertility Investigations for Male and Female before Undertaking Fertility Treatments